Cerebral Aneurysms & SAH
A cerebral aneurysm is an outpouch, or balloon growth from the side of a blood vessel wall in the brain. The aneurysm may grow very large in size, compressing vital nerves in the brain, or may fill with small clots that can break off and travel into the blood vessels of the brain and cause a stroke. However, more commonly an aneurysm may rupture, causing blood to pour out of the blood vessels into the space around the brain, called the subarachnoid space, resulting in a subarachnoid haemorrhage (SAH). SAH is a devastating condition, with many patients dying from the SAH, whilst many others develop severe stroke, with permanent disability.
It is unknown why many people develop an aneurysm and SAH, although there are some well known risk factors including smoking and high blood pressure. In some families, there is a genetic predisposition to aneurysm formation, as there is in some genetic conditions such as polycystic kidney disease.
Ideally, prevention of SAH is better than treatment following SAH, however, most people have no warning signs that they have an aneurysm until it is too late. In people at high risk (eg family history, polycystic kidney disease) then investigations can be performed to determine if they have an aneurysm, and treat the aneurysm before it ruptures.
When a scan is performed for some other reason, and an aneurysm is found, then the question is whether this particular aneurysm will soon rupture. But not all aneurysms rupture, and we do not yet have a test that will tell us which aneurysms will rupture, and which won’t. Therefore, we rely on statistical probability in each and every case.
However, once an aneurysm has ruptured, if the patient survives and makes it to hospital alive, the aneurysm needs to be treated immediately, because after an aneurysm ruptures once, it is most likely that it will soon rupture again. If the patient survives the first rupture, there is no guarantee of survival with subsequent rupture.
Ideally, prevention of SAH is better than treatment following SAH, however, most people have no warning signs that they have an aneurysm until it is too late. In people at high risk (eg family history, polycystic kidney disease) then investigations can be performed to determine if they have an aneurysm, and treat the aneurysm before it ruptures.
When a scan is performed for some other reason, and an aneurysm is found, then the question is whether this particular aneurysm will soon rupture. But not all aneurysms rupture, and we do not yet have a test that will tell us which aneurysms will rupture, and which won’t. Therefore, we rely on statistical probability in each and every case.
However, once an aneurysm has ruptured, if the patient survives and makes it to hospital alive, the aneurysm needs to be treated immediately, because after an aneurysm ruptures once, it is most likely that it will soon rupture again. If the patient survives the first rupture, there is no guarantee of survival with subsequent rupture.
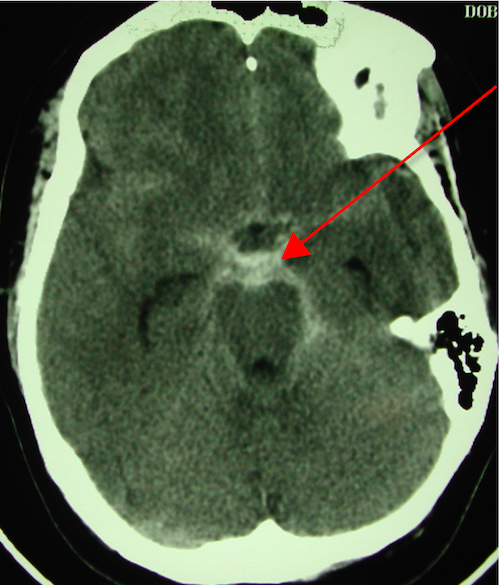
Diagnosis of SAH is made with CT scan, where the blood is seen in the subarachnoid space (red arrow in image below). In some people, the blood is not seen on a CT scan, and then a lumbar puncture is required to diagnose the SAH.
To diagnose the presence of an aneurysm, a scan that demonstrates the anatomy of the blood vessels of the brain is required. Such a scan is called an angiogram. There are 3 types of angiogram. CT angiography and MR angiography are performed in a CT and MRI machine respectively. DSA (Digital subtraction angiography) requires a thin plastic catheter to be inserted into a blood vessel in the groin, and then the catheter travels up to the neck and head arteries, and contrast (a type of dye) is injected into the arteries as Xrays of the brain are taken.
To diagnose the presence of an aneurysm, a scan that demonstrates the anatomy of the blood vessels of the brain is required. Such a scan is called an angiogram. There are 3 types of angiogram. CT angiography and MR angiography are performed in a CT and MRI machine respectively. DSA (Digital subtraction angiography) requires a thin plastic catheter to be inserted into a blood vessel in the groin, and then the catheter travels up to the neck and head arteries, and contrast (a type of dye) is injected into the arteries as Xrays of the brain are taken.
There are advantages and disadvantages to each test type. In essence, DSA is the most accurate, but does carry a small risk, whilst MRA is not quite as accurate, but carries no risk. CTA carries minimal risk, and with improving technology, is nearly as good as DSA.

Treatment of cerebral aneurysms is aimed at eliminating blood flow within the aneurysm, and thus eliminating the risk of rupture.
Clipping of an aneurysm is a microsurgical operation that involves opening the head (craniotomy) and placing a small metal clip across the neck of the aneurysm, in a similar way to tying off a balloon. This provides immediate and long-lasting control of the aneurysm. Clipping of aneurysms is the better treatment option in younger patients, and in aneurysms in certain locations. For example, it is preferable for Middle Cerebral Artery aneurysms to be treated with clipping rather than coiling.
Clipping of an aneurysm is a microsurgical operation that involves opening the head (craniotomy) and placing a small metal clip across the neck of the aneurysm, in a similar way to tying off a balloon. This provides immediate and long-lasting control of the aneurysm. Clipping of aneurysms is the better treatment option in younger patients, and in aneurysms in certain locations. For example, it is preferable for Middle Cerebral Artery aneurysms to be treated with clipping rather than coiling.
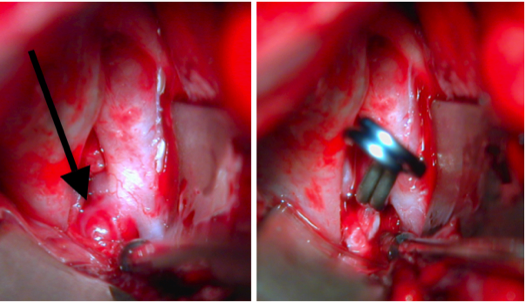
Left - Image shows an aneurysm (black arrow)
Right - Image shows the aneurysm successfully clipped
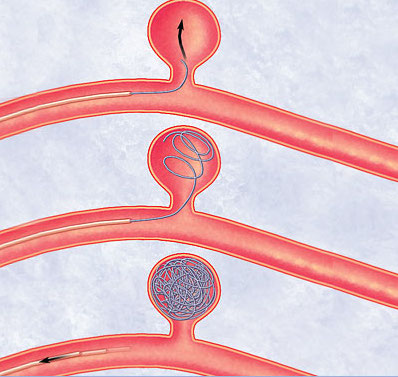
Coiling of an aneurysm involves commencing with a DSA, and then passing small metal coils through the catheter, and directing them into the aneurysm, with the aim of filling the aneurysm with coils so that no blood can get in to the aneurysm. Whilst coiling is not as durable as clipping, it remains the preferred option for certain aneurysms, such as Basilar Artery aneurysms.
The choice of clipping vs coiling depends on the shape of the aneurysm, the aneurysm location (which blood vessel it is on), the number of aneurysms, the patient age, and the experience of the doctors at the treating hospital. Some aneurysms are clearly best clipped, others coiled, and some can be treated with either technique.
The choice of clipping vs coiling depends on the shape of the aneurysm, the aneurysm location (which blood vessel it is on), the number of aneurysms, the patient age, and the experience of the doctors at the treating hospital. Some aneurysms are clearly best clipped, others coiled, and some can be treated with either technique.
After an aneurysm has been treated, the other issue confronting the patient with SAH is vasospasm. Vasospasm is narrowing of brain blood vessels that occurs 3-14 days following SAH, and often results in stroke and death. Approximately 70% of patients with SAH will develop vasospasm. If vasospasm develops, it must be treated aggressively with intravenous fluid treatment and strict blood pressure treatment, as well as special injection via angiography. Patients with severe vasospasm require treatment in the ICU (intensive care unit) until the vasospasm settles, which can take as long as 3 weeks.
If two or more blood-relatives have aneurysms or SAH, then their siblings and children should be offered counselling, to consider performing an angiogram to screen for the presence of aneurysms. Furthermore, all relatives must be strongly cautioned against smoking, and should be advised to see their general practitioner to assess for hypertension (high blood pressure).
If two or more blood-relatives have aneurysms or SAH, then their siblings and children should be offered counselling, to consider performing an angiogram to screen for the presence of aneurysms. Furthermore, all relatives must be strongly cautioned against smoking, and should be advised to see their general practitioner to assess for hypertension (high blood pressure).