Nerve Entrapments
As peripheral nerves travel from the spinal cord and into the limbs (arms & legs), they pass through and under membranes, ligaments and muscles, and across bones and joints. At any of these points, a nerve may become compressed, or squashed, and this results in any of the following problems:
If the condition is left untreated, then the nerve fibres may die off, resulting in permanent disability and pain.
Nerve entrapment is usually due to compression by a fibrous band, or secondary to prolonged pressure on the nerve. For example, after prolonged bed rest, the common peroneal nerve at the knee becomes compressed.
In many cases, the nerve entrapment is secondary to a mass adjacent to the nerve that compresses the nerve. Some commonly encountered masses include ganglion cysts and soft tissue tumours.
The two most common nerve entrapments encountered are Carpal Tunnel Syndrome and Ulnar Neuropathy.
Some other common nerve entrapments encountered are described below.
- pain
- tingling
- pins and needles
- numbness
- weakness
- muscle loss
If the condition is left untreated, then the nerve fibres may die off, resulting in permanent disability and pain.
Nerve entrapment is usually due to compression by a fibrous band, or secondary to prolonged pressure on the nerve. For example, after prolonged bed rest, the common peroneal nerve at the knee becomes compressed.
In many cases, the nerve entrapment is secondary to a mass adjacent to the nerve that compresses the nerve. Some commonly encountered masses include ganglion cysts and soft tissue tumours.
The two most common nerve entrapments encountered are Carpal Tunnel Syndrome and Ulnar Neuropathy.
Some other common nerve entrapments encountered are described below.
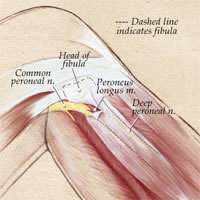
Compression of the Common Peroneal Nerve can occur as it winds around the fibula bone at the knee.
This results in weakness of the foot and toes, especially difficulty lifting the foot up off the ground.
There is also associated numbness on the top of the foot.
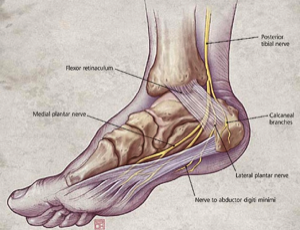
This results from compression of the Tibial Nerve as it passes behind the ankle joint.
It results in pain on the sole of the foot, and may progress to numbness and weakness in the foot.
If severe, then there is loss of all feeling on the sole of the foot, which predisposes to severe ulcers and pressure sores.
Tarsal Tunnel is loosely described as the carpal tunnel of the foot.

This results from compression of the Suprascapular nerve as it passes over the scapula (shoulder blade).
The nerve passes between the scapula and the suprascapular ligament which can compress the nerve.
Symptoms include pain in the shoulder, and weakness of lifting the arm sideways, and rotating the shoulder.
Severe muscle wasting in the back of the shoulder is commonly seen.

This results from compression of the Posterior Interosseous Nerve as it passes through a tunnel (arcade of Frohse) in the supinator muscle in the forearm. This produces pain in the forearm, and significant weakness in wrist and finger extension (pulling the wrist & fingers back).

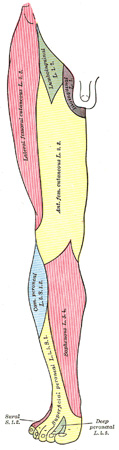
Meralgia Paresthetica
This results from compression of the lateral cutaneous nerve of thigh, which supplies the skin of the lateral thigh. Pain & numbness in the thigh are the usual presenting symptoms. It may be due to obesity, muscle mass, hernias, prostatism, among other things, and the cause should be treated. If no cause is found, then surgical decompression of the nerve may be indicated.
This results from compression of the lateral cutaneous nerve of thigh, which supplies the skin of the lateral thigh. Pain & numbness in the thigh are the usual presenting symptoms. It may be due to obesity, muscle mass, hernias, prostatism, among other things, and the cause should be treated. If no cause is found, then surgical decompression of the nerve may be indicated.
The treatment of nerve entrapment syndromes involves removing the offending cause. In cases of pressure neuropathy (eg peroneal nerve from bed rest), then strict avoidance of pressure to the nerve at the knee may provide time for nerve recovery. If this fails, then surgery is required.
Surgery involves freeing up the nerve by releasing all membranes / bands / bone-spurs that are compressing the nerve.
Following surgery, nerve recovery, if it occurs, may take 3-12 months.
Note that nerve recovery is only possible if the nerve fibres and their insulating coverings have not completely died off before surgical treatment occurs. Therefore, it is extremely important to treat these problems early, before it is too late.
Surgery involves freeing up the nerve by releasing all membranes / bands / bone-spurs that are compressing the nerve.
Following surgery, nerve recovery, if it occurs, may take 3-12 months.
Note that nerve recovery is only possible if the nerve fibres and their insulating coverings have not completely died off before surgical treatment occurs. Therefore, it is extremely important to treat these problems early, before it is too late.