Ulnar Neuropathy
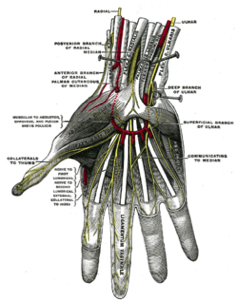
The ulnar nerve is the nerve that controls most fine movements of the fingers, and also supplies sensation to the inside border of the hand.
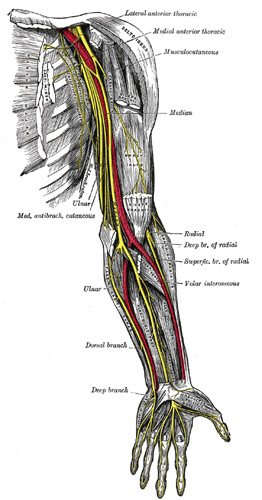
The ulnar nerve takes an odd course down the arm, around the elbow, and then into the forearm and hand. The nerve is commonly compressed behind the elbow. This is made worse by leaning on the elbow with the elbow bent.
When the nerve is compressed, it results in ulnar neuropathy (also known as cubital tunnel syndrome).
Symptoms include:
The diagnosis of ulnar neuropathy requires a careful history and examination from your doctor, and confirmation is made by performing an electrical test called nerve conduction study (NCS) and electromyography (EMG).
When the nerve is compressed, it results in ulnar neuropathy (also known as cubital tunnel syndrome).
Symptoms include:
- numbness in the little and ring fingers, and the inside of the hand
- weakness of the small muscles of the hand.
The diagnosis of ulnar neuropathy requires a careful history and examination from your doctor, and confirmation is made by performing an electrical test called nerve conduction study (NCS) and electromyography (EMG).
Diagnosis of ulnar neuropathy may be quite difficult and complicated because other conditions may mimic the symptoms. Such conditions include cervical disc disease, carpal tunnel syndrome and peripheral neuropathy. In some cases, magnetic resonance imaging (MRI) of the neck and/or elbow may also be required.
The treatment of ulnar neuropathy depends on the symptom severity and duration.
For mild sensory symptoms of short duration, elbow protection is required. This involves strictly avoiding leaning on the elbow. Use of an elbow splint is occasionally useful.
For more severe cases, especially with progressive hand muscle weakness or wasting, then surgery is the recommended treatment.
Surgical treatment of the ulnar nerve at the elbow is performed by many surgeons with simple decompression of the nerve (neurolysis). However, other techniques are available that can provide better results. Professor Gavin Davis has particular expertise in submuscular transposition (SMT) of the nerve, which often provides the best long term results in treatment of ulnar neuropathy. SMT is also used when neurolysis fails to work.
Prof Davis will usually refer patients for a course of formal hand therapy following the surgery. This assists with wound healing, scar management and hand functional recovery.
The treatment of ulnar neuropathy depends on the symptom severity and duration.
For mild sensory symptoms of short duration, elbow protection is required. This involves strictly avoiding leaning on the elbow. Use of an elbow splint is occasionally useful.
For more severe cases, especially with progressive hand muscle weakness or wasting, then surgery is the recommended treatment.
Surgical treatment of the ulnar nerve at the elbow is performed by many surgeons with simple decompression of the nerve (neurolysis). However, other techniques are available that can provide better results. Professor Gavin Davis has particular expertise in submuscular transposition (SMT) of the nerve, which often provides the best long term results in treatment of ulnar neuropathy. SMT is also used when neurolysis fails to work.
Prof Davis will usually refer patients for a course of formal hand therapy following the surgery. This assists with wound healing, scar management and hand functional recovery.