Trigeminal Neuralgia
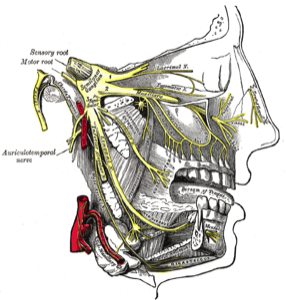
The trigeminal nerve arises from the pons in the brainstem, and travels through the fluid space around the brain called the basal cisterns. It then travels through a membrane in the wall of the cavernous sinus before leaving the base of the skull through a bony opening, and then travels to the face where its three branches supply sensation to the skin and eye, as will as supplying some muscles of the jaw.
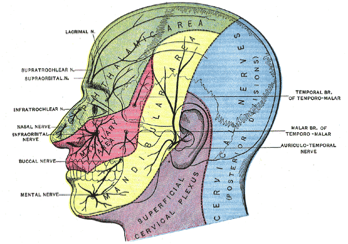
If the nerve is compressed in the basal cistern (the cerebello-pontine angle, CPA), then trigeminal neuralgia (tic douloureux) may develop.
This results in severe, lancinating-like pain in the face, usually in the distribution of one of the three branches of the trigeminal nerve.
The most common cause of trigeminal neuralgia is compression of the nerve in the CPA by a loop of an artery. An artery that compresses the nerve as it leaves the pons at the root entry zone (REZ) causes the nerve insulation (myelin) to break down, and this results in excessive electrical firing of the nerve which causes the severe pain (see image below left).
Other causes of trigeminal neuralgia include multiple sclerosis, tumours, cysts, trauma or aneurysms.
Investigation of trigeminal neuralgia requires an MRI scan. The MRI scan is used to exclude the presence of a mass such as a tumour.
Treatment of trigeminal neuralgia begins with the use of anti-convulsant medication such as phenytoin, carbamazepine, valproate or gabapentin. In many people, this will control symptoms.
If medication fails to control the pain, or if the effects of medication wear off, then surgery is required.
Surgery can take one of two types, Ablative or Microvascular Decompression.
Ablative surgery involves partially or completely injuring or destroying the nerve to numb it, and thus reduce the pain. Whilst this is the first line treatment in people with multiple sclerosis, it is rarely recommended for patients with typical trigeminal neuralgia that is due to vascular compression. Ablation results in permanent numbness in the face, and does place the eye at risk. Recurrence of pain is not uncommon.
Some ablative techniques employed include radiofrequency ablation, glycerol injection, balloon compression and nerve section.
Other causes of trigeminal neuralgia include multiple sclerosis, tumours, cysts, trauma or aneurysms.
Investigation of trigeminal neuralgia requires an MRI scan. The MRI scan is used to exclude the presence of a mass such as a tumour.
Treatment of trigeminal neuralgia begins with the use of anti-convulsant medication such as phenytoin, carbamazepine, valproate or gabapentin. In many people, this will control symptoms.
If medication fails to control the pain, or if the effects of medication wear off, then surgery is required.
Surgery can take one of two types, Ablative or Microvascular Decompression.
Ablative surgery involves partially or completely injuring or destroying the nerve to numb it, and thus reduce the pain. Whilst this is the first line treatment in people with multiple sclerosis, it is rarely recommended for patients with typical trigeminal neuralgia that is due to vascular compression. Ablation results in permanent numbness in the face, and does place the eye at risk. Recurrence of pain is not uncommon.
Some ablative techniques employed include radiofrequency ablation, glycerol injection, balloon compression and nerve section.
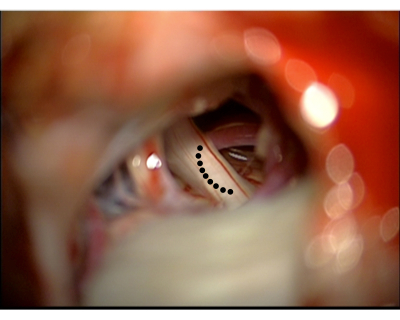
Intraoperative microscopic view demonstrates the trigeminal nerve compressed by the adjacent artery. The black dots represent the site of the nerve compression by the loop of the artery lying deep to the nerve.
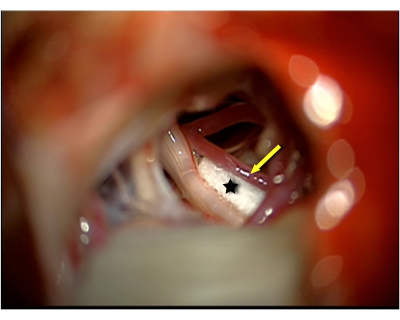
Intraoperative microscopic view demonstrates the artery (yellow arrow) that was marked by the black dots in the image on the left, now separated off the trigeminal nerve by a small pledget of teflon (black star).

As the cause of trigeminal neuralgia is usually compression of the nerve at the REZ by a loop of an artery, the best treatment is to separate the artery off the nerve, which affords excellent long term cure in most patients.
This operation involves opening the skull behind the ear, and exposing the Cerebello-pontine Angle using microsurgical techniques. The trigeminal nerve is exposed, and the offending artery is separated off the nerve. To stop the artery from falling back on the nerve, a small piece of teflon is placed around the artery. See images above.
If you have trigeminal neuralgia that responds poorly to medications, or if the medications have significant side effects, then Professor Gavin Davis will assess whether this procedure is suitable for you, based on the clinical presentation and the MRI findings.